
Consolidation of physician services into larger groups owned by hospitals and health care systems is driving up the cost of care in workers’ compensation, according to a new study by the Workers’ Compensation Research Institute.
“Medical markets are increasingly concentrated,” said John Ruser, WCRI president and chief executive officer, in a statement. “This means that patients are more likely to be treated by physicians at sites owned by hospitals and health systems. This raises a policy concern that the increasing concentration of medical providers may lead to higher payments for medical care without corresponding improvements in patient outcomes.”
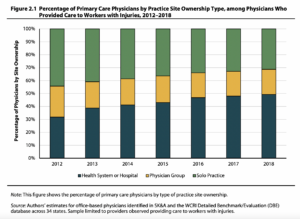
The study found that from 2012 to 2018 the percentage of physicians practicing at sites owned by hospitals or health systems increased to 49% from 32% for primary care physicians, and to 35% from 18% for orthopedic surgeons.
 This “vertical integration” of the industry increased the average payment per procedure by 8% overall, or $29 per procedure. But costs increased more in states that don’t use fee schedules to regulate prices charged for treating injured workers. In those states, payments per procedure increased an average of $91 because of vertical integration, the study says.
This “vertical integration” of the industry increased the average payment per procedure by 8% overall, or $29 per procedure. But costs increased more in states that don’t use fee schedules to regulate prices charged for treating injured workers. In those states, payments per procedure increased an average of $91 because of vertical integration, the study says.
WCRI said the study, conducted by researchers Bogdan Savych and Olesya Fomenko, is the first to study the cost of vertical integration in workers’ compensation.
The study said most of the increase in costs was driven by changes in the frequency and mix of services provided, known as utilization. Vertical integration increased the price of each procedure provided by only 2%.
The study says a substantial amount of research has found that fewer physicians are employed in sole practice and more are employees of health systems hospitals. Advocates for consolidation say it leads to more frequent use of best practices and better coordination of care, but skeptics say that consolidation reduces competition and leads to higher prices for medical care.
WCRI, looking specifically at primary care physicians who treat injured workers, found that more than 44% were in sole practice in 2012 and only 31% were in sole practice in 2018. For orthopedic surgeons, the share in sole practice declined from 41% to 27% during that period.
In the meantime, the share of primary care physicians employed by hospitals are health systems climbed from 33% to 49% and the share of orthopedic surgeons working for hospitals and health systems climbed from 18% to 35%.
The WCRI researchers found the cost of vertical integration varied largely by location and type of provider. The study found the impact of consolidation was greatest in states without fee schedules.
Vertical integration in those states led to 12% increases in payments per procedure, a 14% in payments per service type and an 11% increase in payments per day of care. For states with fee schedules, vertical integration led to payment increases ranging from 7% to 9% in each category.
“We can expect that when a state has a fixed-amount fee schedule, there are fewer opportunities for vertically-integrated providers to affect prices,” the study says. “However, prices may be more responsive to changes in the market power of providers in states without fixed-amount fee schedules.”
The study did not include any information on whether the higher prices charged led to better outcomes for workers’ compensation patients, but suggested more research is needed in that area.
Was this article valuable?
Here are more articles you may enjoy.
 Navigators Can’t Parse ‘Additional Insured’ Policy Wording in Georgia Explosion Case
Navigators Can’t Parse ‘Additional Insured’ Policy Wording in Georgia Explosion Case  Tesla Sued Over Crash That Trapped, Killed Massachusetts Driver
Tesla Sued Over Crash That Trapped, Killed Massachusetts Driver  LA County Told to Pause $4B in Abuse Payouts as DA Probes Fraud Claims
LA County Told to Pause $4B in Abuse Payouts as DA Probes Fraud Claims  Credit Suisse Nazi Probe Reveals Fresh SS Ties, Senator Says
Credit Suisse Nazi Probe Reveals Fresh SS Ties, Senator Says 
Want to stay up to date?
Get the latest insurance news
sent straight to your inbox.